A 65 year old POSTURAL DIZZINESS AND VOMITING
65Year old female POSTURAL DIZZINESS AND VOMITING
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio.

.jpeg)
.jpeg)
.jpeg)


63 year old housewife from Nalgonda
Chief complaints- Vomiting 5 episodes 3 days ago
History of present illness-
Patient was apparently alright 1 year back then developed vomiting associated with giddiness and pain. she came to our hospital and vomiting subsided with treatment. She was asked to take Vertin 24 (betahistine) at discharge. she took the medication for 3 months and then stopped after consulting with her physician. She had mild episodes of vomiting for the next months until 3 days back when she had 5 episodes (severe)
Vomiting- non projectile, contents were food/watery. there was no blood present in the vomitus. no temporal association with meal timings was noticed. it was associated with giddiness and colicky, non radiating pain in the epigastrium, present only during the episode. Not associated with fever, headache, diarrhoea or constipation.
Frequency of stools are normal but volume is decreased due to less food intake out of fear of vomiting.
No history of- abdominal distention, heart burn, acidity, excessive flatulence, jaundice.
Giddiness- there was no history of headache, trauma, fall, stroke, aural fullness, tinnitus, no positional variation or triggering factors (starts randomly). no aggravating factors. relieved with medications.
Past history-
Patient is a known case of hypertension since 5 years, is on medication Telma 40.
No history of tuberculosis, diabetes mellitus, stroke.
Personal history-
Mixed diet
Reduced appetite
Adequate sleep
Bowel movements are of normal frequency but reduced volume
Bladder movements are normal
No addictions or allergies
Occasionally drinks toddy.
Daily routine (premorbid)
0500- wakes up
0500-0600- gets ready
0730- Chai + bun
0730- 1300- stays indoors, doesn't do much
1100- Rice+ curry
1300- Buttermilk+rice
1300-2000- stays indoors, doesn't do much
2000- Rice+curry
morbid changes- doesn't eat much due to fear of vomiting, however, small meals are consumed regularly.
Family history- No similar complaints in the family. no history of HTN or DM in the family.
General examination-
Patient is concious coheret cooperative and oriented to time place and person.
built- average
nourishment- average
Pallor is present, icterus, cyanosis, clubbing, lymphadenopathy or edema are absent.
Temperature- Afebrile
PR- 78 bpm, regular, normal volume, normal character, no radioradial delay, no radiofemoral delay.
RR- 17 cpm
BP- 130/80 mmHg
Decreased range of motion of neck flexion
Fixed flexion deformity of bilateral knees with left being more then right
.jpeg)
.jpeg)
Systemic examination-
Per Abdomen-
Inspectionshape- flat
flanks- empty
umbilicus- inverted
striae gravidarum present.
normal movements with respiration
no visible pulsations, peristalsis, or hernial orifices
abdominal girth-
palpation-
no local rise of temperature or tenderness in any quadrant. no guarding or rigidity. liqver and spleen were non palpable.
Percussion- no shifting dullness or fluid thrill present.
Auscultation- Bowel sounds heard.
Central nervous system-
Concious, Coherent, Cooperative, orientated to time, place, person
memory- recent memory impaired
speech- Normal
Gait- short steps with broad bas
cranial nerves-
1- Smell intact
2- Counting fingers+ menace reflex+
3, 4, 6-External ocular movements- full and free, accomodation reflex +
5- Sensations on face normal. able to open jaw against resistance.
7- Movements of face normal
8- Rinne's test negative with 512, Weber's test negative
9, 10, 11- gag reflex on both sides present, no uvula deviation, normal swallowing, shrugging of shoulders against resistance+
12- No deviation of tongue.
Motor-
RIGHT LEFT
Bulk- UL 26cm 26cm
LL 41cm 39cm
Tone- UL N N
LL bilateral hypertonia (quadriceps and gastrocnemius)
Power- UL 5 5
LL 4 4
Reflexes- Biceps 3 2
Triceps 2 2
Supinator 2 2
Knee 1 1
Ankle 1 1
Plantar 1 1
sensory- UL LL
Fine touch- N decreased
crude touch- N decreased
pain- N N
temperature-
vibration sense- N decreased
proprioception- N decreased
proprioception- N decreased
2 point discrimination 20cm unable to ellicit
stereognosis intact
Cerebellar-
Finger nose test- slow
Knee heel test- slow
Dysdiadochokinesia- slow
Neck stiffness- present
kernig sign- absent
bruzdinki sign- absent
Romberg test- positive
cranial nerves-
1- Smell intact
2- Counting fingers+ menace reflex+
3, 4, 6-External ocular movements- full and free, accomodation reflex +
5- Sensations on face normal. able to open jaw against resistance.
7- Movements of face normal
8- Rinne's test negative with 512, Weber's test negative
9, 10, 11- gag reflex on both sides present, no uvula deviation, normal swallowing, shrugging of shoulders against resistance+
12- No deviation of tongue.
Motor-
RIGHT LEFT
Bulk- UL 26cm 26cm
LL 41cm 39cm
Tone- UL N N
LL bilateral hypertonia (quadriceps and gastrocnemius)
Power- UL 5 5
LL 4 4
Reflexes- Biceps 3 2
Triceps 2 2
Supinator 2 2
Knee 1 1
Ankle 1 1
Plantar 1 1
sensory- UL LL
Fine touch- N decreased
crude touch- N decreased
pain- N N
temperature-
vibration sense- N decreased
proprioception- N decreased
proprioception- N decreased
2 point discrimination 20cm unable to ellicit
stereognosis intact
Cerebellar-
Finger nose test- slow
Knee heel test- slow
Dysdiadochokinesia- slow
Neck stiffness- present
kernig sign- absent
bruzdinki sign- absent
Romberg test- positive
Cardiovascular system- S1, S2 heard, no thrills or murmurs
Respiratory system- Bilateral air entry present, normal vesicular breath sounds heard, no added sounds.
Provisional diagnosis- vertebrobasillar insufficiency
Differential diagnosis- benign paroxysmal positional vertigo, meniers disease, vestibular neuritis, cerebellar palsy, multiple sclerosis, labrynthitis
Investigations- 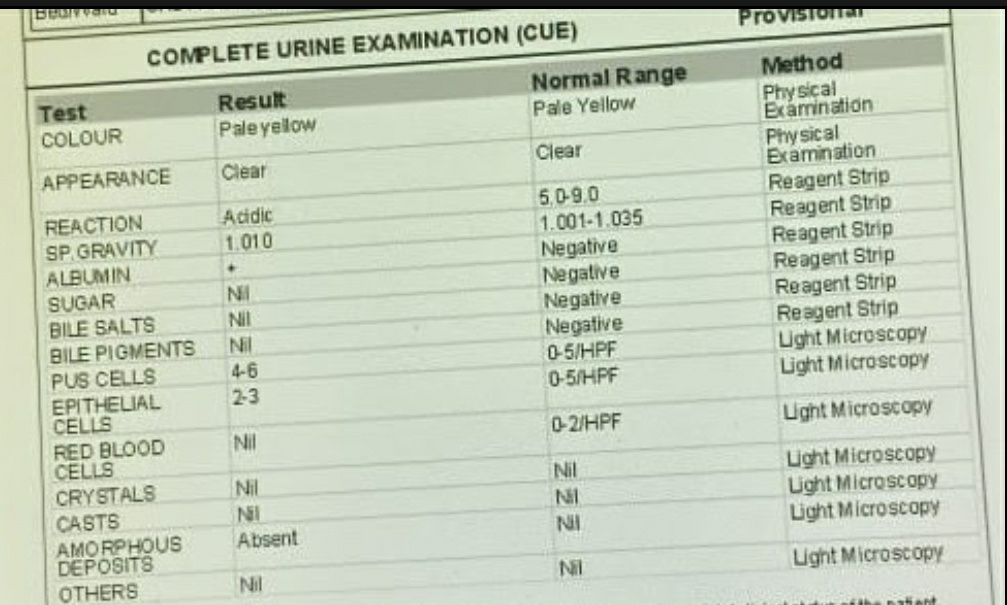





Treatment-
INJ OFER 4mg IV
INJ PAN 40mg IV
TAB TELMA 40mg PO
TAB PREGAM mg
TAB SHELCAL CT
TAB VIT D2
TAB SUPADYN
IV FLUID NS PO OD
BP, PR, TEMP motoring
Comments
Post a Comment